


Estrogen dominance and inadequate levels of progesterone can cause fertility issues and problems during pregnancy. The standard dose of estradiol valerate is 6 mg daily (Cobo et al., 2012), although different step up protocolsmimicking the rising estradiol levels of a NCare also frequently used (Soares et al., 2005; Escrib et al., 2006; van de Vijver et al., 2014). 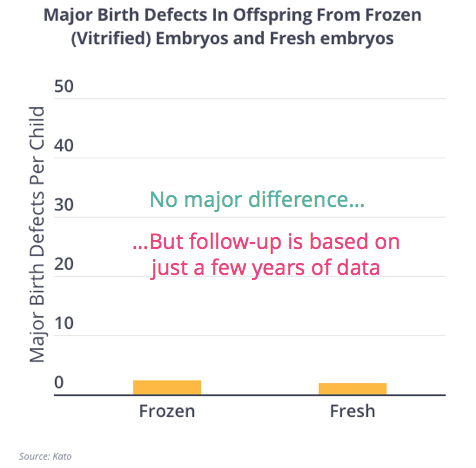 Due to prolonged half-life of hCG used as trigger, it makes biological sense that no LPS may be needed, although not all researchers agree (Kim et al., 2014). Conversely, HRT FET cycles without GnRH agonist co-treatment seem to be more patient-friendly given the avoidance of the cost and potential side effects associated with these drugs. Although originally developed to allow embryo transfers in recipients of donated oocytes, the HRT protocol has proven to be successful in the general population as well (Younis et al., 1996), thus extending its advantages in terms of minimal monitoring and easy scheduling to those performing IVF overall.
Due to prolonged half-life of hCG used as trigger, it makes biological sense that no LPS may be needed, although not all researchers agree (Kim et al., 2014). Conversely, HRT FET cycles without GnRH agonist co-treatment seem to be more patient-friendly given the avoidance of the cost and potential side effects associated with these drugs. Although originally developed to allow embryo transfers in recipients of donated oocytes, the HRT protocol has proven to be successful in the general population as well (Younis et al., 1996), thus extending its advantages in terms of minimal monitoring and easy scheduling to those performing IVF overall.  In most cases, the transfer occurs in the following menstrual cycle the next month. Murray MJ, Meyer WR, Zaino RJ, Lessey BA, Novotny DB, Ireland K, Zeng D, Fritz MA. We suggest not to administer hCG when a spontaneous LH surge is detected, given the previously noted potential association with a detrimental outcome (Fatemi et al., 2010), even though it has not been confirmed in a recent post hoc analysis of the ANTARCTICA trial (Groenewoud et al., 2017). Decidualization, the secretory transformation that the endometrial stromal compartment undergoes to accommodate pregnancy, plays an important role in receptivity as it is thought to contribute to the active selection of embryos attempting implantation (Brosens et al., 2014). A randomised study, Delaying the initiation of progesterone supplementation until the day of fertilization does not compromise cycle outcome in patients receiving donated oocytes: a randomized study, European IVF-Monitoring Consortium (EIM), European Society of Human Reproduction and Embryology (ESHRE), Assisted reproductive technology in Europe, 2011: results generated from European registers by ESHRE, Fresh versus frozen embryo transfer: backing clinical decisions with scientific and clinical evidence, Cryopreserved-thawed human embryo transfer: spontaneous natural cycle is superior to human chorionic gonadotropin-induced natural cycle, Both slowly developing embryos and a variable pace of luteal endometrial progression may conspire to prevent normal birth in spite of a capable embryo, Intrauterine insemination: effect of the temporal relationship between the luteinizing hormone surge, human chorionic gonadotrophin administration and insemination on pregnancy rates, Cycle regimens for frozen-thawed embryo transfer, Outcomes of natural cycles versus programmed cycles for 1677 frozen-thawed embryo transfers, Endometrial preparation for women undergoing embryo transfer with frozen embryos or embryos derived from donor oocytes, Non-synchronized endometrium and its correction in non-ovulatory cryopreserved embryo transfer cycles, Mid-cycle serum levels of endogenous LH are not associated with the likelihood of pregnancy in artificial frozen-thawed embryo transfer cycles without pituitary suppression, What is the optimal means of preparing the endometrium in frozen-thawed embryo transfer cycles? You should not rely solely on this information. In current daily practice, different FET preparation methods and timing strategies are used. What is the preferred method for timing natural cycle frozen-thawed embryo transfer? The goal of fertility-sparing treatment (FST) for patients desiring future fertility with EMCA, and its precursor EH, is to clear the affected tissue and revert to normal endometrial function. Though some studies have reported increased D14 TSH after fresh ET, few studies have focused on the impact of D14 TSH after frozen-thawed embryo transfer (FET) on clinical outcomes, the ideal D14 TSH after FET, whether this parameter matters for clinical outcomes. Background: This study aimed to explore the relationship between serum oestrogen (E 2) levels before endometrial transformation and pregnancy outcomes of hormone replacement therapy-frozen embryo transfer (HRT-FET) cycles, which has been investigated for years without any consensus. As only a few high quality RCTs on the optimal preparation for FET are available in the existing literature, no definitive conclusion for benefit of one protocol over the other can be drawn so far. Purpose Estrogen is well-known for preparing uterine receptivity. When progesterone supplementation in HRT cycles is initiated 3 days before the cleavage embryo transfer, excellent pregnancy rates of up to 40.5% occur (Givens et al., 2009). However, endocrine cycle monitoring was not performed in that study, and the incidence of premature ovulation was not reported.
In most cases, the transfer occurs in the following menstrual cycle the next month. Murray MJ, Meyer WR, Zaino RJ, Lessey BA, Novotny DB, Ireland K, Zeng D, Fritz MA. We suggest not to administer hCG when a spontaneous LH surge is detected, given the previously noted potential association with a detrimental outcome (Fatemi et al., 2010), even though it has not been confirmed in a recent post hoc analysis of the ANTARCTICA trial (Groenewoud et al., 2017). Decidualization, the secretory transformation that the endometrial stromal compartment undergoes to accommodate pregnancy, plays an important role in receptivity as it is thought to contribute to the active selection of embryos attempting implantation (Brosens et al., 2014). A randomised study, Delaying the initiation of progesterone supplementation until the day of fertilization does not compromise cycle outcome in patients receiving donated oocytes: a randomized study, European IVF-Monitoring Consortium (EIM), European Society of Human Reproduction and Embryology (ESHRE), Assisted reproductive technology in Europe, 2011: results generated from European registers by ESHRE, Fresh versus frozen embryo transfer: backing clinical decisions with scientific and clinical evidence, Cryopreserved-thawed human embryo transfer: spontaneous natural cycle is superior to human chorionic gonadotropin-induced natural cycle, Both slowly developing embryos and a variable pace of luteal endometrial progression may conspire to prevent normal birth in spite of a capable embryo, Intrauterine insemination: effect of the temporal relationship between the luteinizing hormone surge, human chorionic gonadotrophin administration and insemination on pregnancy rates, Cycle regimens for frozen-thawed embryo transfer, Outcomes of natural cycles versus programmed cycles for 1677 frozen-thawed embryo transfers, Endometrial preparation for women undergoing embryo transfer with frozen embryos or embryos derived from donor oocytes, Non-synchronized endometrium and its correction in non-ovulatory cryopreserved embryo transfer cycles, Mid-cycle serum levels of endogenous LH are not associated with the likelihood of pregnancy in artificial frozen-thawed embryo transfer cycles without pituitary suppression, What is the optimal means of preparing the endometrium in frozen-thawed embryo transfer cycles? You should not rely solely on this information. In current daily practice, different FET preparation methods and timing strategies are used. What is the preferred method for timing natural cycle frozen-thawed embryo transfer? The goal of fertility-sparing treatment (FST) for patients desiring future fertility with EMCA, and its precursor EH, is to clear the affected tissue and revert to normal endometrial function. Though some studies have reported increased D14 TSH after fresh ET, few studies have focused on the impact of D14 TSH after frozen-thawed embryo transfer (FET) on clinical outcomes, the ideal D14 TSH after FET, whether this parameter matters for clinical outcomes. Background: This study aimed to explore the relationship between serum oestrogen (E 2) levels before endometrial transformation and pregnancy outcomes of hormone replacement therapy-frozen embryo transfer (HRT-FET) cycles, which has been investigated for years without any consensus. As only a few high quality RCTs on the optimal preparation for FET are available in the existing literature, no definitive conclusion for benefit of one protocol over the other can be drawn so far. Purpose Estrogen is well-known for preparing uterine receptivity. When progesterone supplementation in HRT cycles is initiated 3 days before the cleavage embryo transfer, excellent pregnancy rates of up to 40.5% occur (Givens et al., 2009). However, endocrine cycle monitoring was not performed in that study, and the incidence of premature ovulation was not reported.  Once the proliferation of the endometrium with the administration of estrogens is considered sufficient, progesterone is initiated to promote the final phase of endometrial preparation prior to embryo transfer. Cryopreserved embryo transfer in an artificial cycle: is GnRH agonist down-regulation necessary? . No progesterone production can result in estrogen dominance. apOj-&FPKg|` V$
eCollection
Once the proliferation of the endometrium with the administration of estrogens is considered sufficient, progesterone is initiated to promote the final phase of endometrial preparation prior to embryo transfer. Cryopreserved embryo transfer in an artificial cycle: is GnRH agonist down-regulation necessary? . No progesterone production can result in estrogen dominance. apOj-&FPKg|` V$
eCollection 
 a Day 5 embryo on LH + 6).
a Day 5 embryo on LH + 6).  What the normal range for estradiol levels are in an IVF cycle, What to expect the level to be on any given day, Poor responders: Patients in the bottom 10th percentile for estrogen levels, Normal responders: Patients in the 50th percentile for estrogen levels, High responders: Patients in the 90th percentile for estrogen levels, It thickens the uterine lining in preparation for embryo implantation, It helps fertility doctors monitor your response to IVF stimulation and predict the number of oocytes you might get at the oocyte retrieval, It plays an important role in endometrial receptivity and pregnancy maintenance. Groenewoud ER, Cohlen BJ, Al-Oraiby A, Brinkhuis EA, Broekmans FMJ, de Bruin JP, van den Dool G, Fleisher K, Friederich J, Goddijn M et al. Transferring an embryo in the setting of OHSS can significantly worsen the condition and put you at risk for more complications. 254 0 obj
<>stream
The impact of legally restricted embryo transfer and reimbursement policy on cumulative delivery rate after treatment with assisted reproduction technology, Endometrial thickness and serum oestradiol concentrations as predictors of outcome in oocyte donation, Timing of hCG administration does not affect pregnancy rates in couples undergoing intrauterine insemination using clomiphene citrate, Fresh embryo transfer versus frozen embryo transfer in in vitro fertilization cycles: a systematic review and meta-analysis, Freeze-all policy: fresh vs. frozen-thawed embryo transfer, The luteal phase defect: the relative frequency of, and encouraging response to, treatment with vaginal progesterone, The endometrial receptivity array for diagnosis and personalized embryo transfer as a treatment for patients with repeated implantation failure, Replacement of frozen - thawed embryos in artificial and natural cycles: a prospective semi-randomized study, A human in vivo model for the luteoplacental shift, Pharmacokinetics of percutaneous estradiol: a crossover study using a gel and a transdermal system in comparison with oral micronized estradiol, Evidence of impaired endometrial receptivity after ovarian stimulation for in vitro fertilization: a prospective randomized trial comparing fresh and frozen-thawed embryo transfer in normal responders, Contrasting patterns in in vitro fertilization pregnancy rates among fresh autologous, fresh oocyte donor, and cryopreserved cycles with the use of day 5 or day 6 blastocysts may reflect differences in embryo-endometrium synchrony, Progesterone replacement with vaginal gel versus i.m. In such cases, it is likely better to take into account the expected embryonic stage at the moment of transfer instead of the stage in which the embryo was cryopreserved (Cercas et al., 2012; Jin et al., 2013; van de Vijver et al., 2016). Soares SR, Troncoso C, Bosch E, Serra V, Simn C, Remoh J, Pellicer A. Testart J, Frydman R, Feinstein MC, Thebault A, Roger M, Scholler R. Toms C, Alsbjerg B, Martikainen H, Humaidan P. Tournaye H, Sukhikh GT, Kahler E, Griesinger G. van de Vijver A, Drakopoulos P, Polyzos NP, Van Landuyt L, Mackens S, Santos-Ribeiro S, Vloeberghs V, Tournaye H, Blockeel C. van de Vijver A, Polyzos NP, Van Landuyt L, De Vos M, Camus M, Stoop D, Tournaye H, Blockeel C. van de Vijver A, Polyzos NP, Van Landuyt L, Mackens S, Stoop D, Camus M, De Vos M, Tournaye H, Blockeel C. Veleva Z, Tiitinen A, Vilska S, Hydn-Granskog C, Toms C, Martikainen H, Tapanainen JS. Hence, future research should compare both the pregnancy and neonatal outcomes between HRT and true NC FET. If the results are low, it i Read More These anovulatory cycles are most common among women between the ages of 30 and 50 and in women with secondary conditions which affect ovulation, such as polycystic ovary syndrome and endometriosis. Conversely, given that a previous meta-analysis has associated endometrial thickness 7 mm in fresh IVF cycles with a lower chance of pregnancy, this cut-off value is generally extrapolated to FET as well; however, the actual value of this arbitrary cut-off and whether the same limit can be extrapolated to frozen cycles requires further research (Dain et al., 2013; Kasius et al., 2014). Make an appointment with Dr. Robles to discuss your fertility options today! However, there is no RCT comparing IM and vaginal routes in HRT FET cycles. At the basic research level, the evidence points toward the NC being superior to HRT.
What the normal range for estradiol levels are in an IVF cycle, What to expect the level to be on any given day, Poor responders: Patients in the bottom 10th percentile for estrogen levels, Normal responders: Patients in the 50th percentile for estrogen levels, High responders: Patients in the 90th percentile for estrogen levels, It thickens the uterine lining in preparation for embryo implantation, It helps fertility doctors monitor your response to IVF stimulation and predict the number of oocytes you might get at the oocyte retrieval, It plays an important role in endometrial receptivity and pregnancy maintenance. Groenewoud ER, Cohlen BJ, Al-Oraiby A, Brinkhuis EA, Broekmans FMJ, de Bruin JP, van den Dool G, Fleisher K, Friederich J, Goddijn M et al. Transferring an embryo in the setting of OHSS can significantly worsen the condition and put you at risk for more complications. 254 0 obj
<>stream
The impact of legally restricted embryo transfer and reimbursement policy on cumulative delivery rate after treatment with assisted reproduction technology, Endometrial thickness and serum oestradiol concentrations as predictors of outcome in oocyte donation, Timing of hCG administration does not affect pregnancy rates in couples undergoing intrauterine insemination using clomiphene citrate, Fresh embryo transfer versus frozen embryo transfer in in vitro fertilization cycles: a systematic review and meta-analysis, Freeze-all policy: fresh vs. frozen-thawed embryo transfer, The luteal phase defect: the relative frequency of, and encouraging response to, treatment with vaginal progesterone, The endometrial receptivity array for diagnosis and personalized embryo transfer as a treatment for patients with repeated implantation failure, Replacement of frozen - thawed embryos in artificial and natural cycles: a prospective semi-randomized study, A human in vivo model for the luteoplacental shift, Pharmacokinetics of percutaneous estradiol: a crossover study using a gel and a transdermal system in comparison with oral micronized estradiol, Evidence of impaired endometrial receptivity after ovarian stimulation for in vitro fertilization: a prospective randomized trial comparing fresh and frozen-thawed embryo transfer in normal responders, Contrasting patterns in in vitro fertilization pregnancy rates among fresh autologous, fresh oocyte donor, and cryopreserved cycles with the use of day 5 or day 6 blastocysts may reflect differences in embryo-endometrium synchrony, Progesterone replacement with vaginal gel versus i.m. In such cases, it is likely better to take into account the expected embryonic stage at the moment of transfer instead of the stage in which the embryo was cryopreserved (Cercas et al., 2012; Jin et al., 2013; van de Vijver et al., 2016). Soares SR, Troncoso C, Bosch E, Serra V, Simn C, Remoh J, Pellicer A. Testart J, Frydman R, Feinstein MC, Thebault A, Roger M, Scholler R. Toms C, Alsbjerg B, Martikainen H, Humaidan P. Tournaye H, Sukhikh GT, Kahler E, Griesinger G. van de Vijver A, Drakopoulos P, Polyzos NP, Van Landuyt L, Mackens S, Santos-Ribeiro S, Vloeberghs V, Tournaye H, Blockeel C. van de Vijver A, Polyzos NP, Van Landuyt L, De Vos M, Camus M, Stoop D, Tournaye H, Blockeel C. van de Vijver A, Polyzos NP, Van Landuyt L, Mackens S, Stoop D, Camus M, De Vos M, Tournaye H, Blockeel C. Veleva Z, Tiitinen A, Vilska S, Hydn-Granskog C, Toms C, Martikainen H, Tapanainen JS. Hence, future research should compare both the pregnancy and neonatal outcomes between HRT and true NC FET. If the results are low, it i Read More These anovulatory cycles are most common among women between the ages of 30 and 50 and in women with secondary conditions which affect ovulation, such as polycystic ovary syndrome and endometriosis. Conversely, given that a previous meta-analysis has associated endometrial thickness 7 mm in fresh IVF cycles with a lower chance of pregnancy, this cut-off value is generally extrapolated to FET as well; however, the actual value of this arbitrary cut-off and whether the same limit can be extrapolated to frozen cycles requires further research (Dain et al., 2013; Kasius et al., 2014). Make an appointment with Dr. Robles to discuss your fertility options today! However, there is no RCT comparing IM and vaginal routes in HRT FET cycles. At the basic research level, the evidence points toward the NC being superior to HRT.  However in HRT FET cycles, as no corpus luteum and, hence, no endogenous progesterone productionis present, the best moment remains to be elucidated. Dain L, Bider D, Levron J, Zinchenko V, Westler S, Dirnfeld M. Dal Prato L, Borini A, Cattoli M, Bonu MA, Sciajno R, Flamigni C. Daz-Gimeno P, Horcajadas JA, Martnez-Conejero JA, Esteban FJ, Alam P, Pellicer A, Simn C. Edgell TA, Rombauts LJF, Salamonsen LA. Sorry you're going through this, is your RE concerned? In addition, previous studies have shown low estradiol levels are associated with decreased implantation rates and clinical pregnancy rates. is funded by the Research Fund of Flanders (FWO). Objective: To explore whether a high serum estradiol (E2) level before progesterone administration adversely affects the pregnancy outcomes of frozen-thawed embryo transfer (FET) cycles. In terms of embryo transfer timing, we propose to start progesterone intake on the theoretical day of oocyte retrieval in HRT and to perform blastocyst transfer at hCG + 7 or LH + 6 in modified or true NC, respectively. Recently, a large, multi-center, non-inferiority trial studying modified NC versus HRT has failed to show any significant difference in live birth, clinical or ongoing pregnancy rates (Groenewoud et al., 2016). WebAn estrogen level above 3,500 pg/mL is considered high and a risk factor for adverse effects. However, more data are needed to confirm the safety and efficacy of oral dydrogesterone in HRT FET. A difference in the timing of FET in true versus modified NC could be considered, as ovulation occurs 3648 h after hCG administration but varies from 24 to 56 h after a spontaneous LH surge (Kosmas et al., 2007). Keltz MD, Jones EE, Duleba AJ, Polcz T, Kennedy K, Olive DL. WebWhen progesterone supplementation in HRT cycles is initiated 3 days before the cleavage embryo transfer, excellent pregnancy rates of up to 40.5% occur (Givens et al., 2009). However, this study did not assess the potential benefit of FET performed without exogenous ovulation triggering and concerns were raised due to the overall low success rate reported and the high miscarriage rates (Hreinsson et al., 2016). We have observed that in studies assessing the optimal preparation for FET, embryo transfer timing is often described vaguely or confusingly. Things that can elevate a Day 3 estradiol include: If you intend to start an IVF cycle and your estrogen levels are elevated, we generally will delay starting until we get the values back to a normal range. Exogenous mild ovarian stimulation instead of direct estrogen supplementation has been proposed aiming to increase the circulation of serum estrogen and potentially enhance endometrial receptivity. Can You Get Pregnant With High Estrogen Levels? Scott R, Navot D, Liu HC, Rosenwaks Z. Scott RT, Ross B, Anderson C, Archer DF. Approximately 15% of patients treated with FST will have a live birth without the need for assisted reproductive technology (ART). and C.B. Save my name, email, and website in this browser for the next time I comment. (;G\? This is a more common practice for logistical reasons and because this method is more likely to result in a live birth. A Cochrane Database Review concluded that starting progesterone at a time equivalent to the day of or the day after oocyte retrieval (OR) results in a significantly higher pregnancy rate than if progesterone is initiated a day earlier than the day equivalent to OR (Glujovsky et al., 2010). Estrogen level monitoring in artificial frozen-thawed embryo transfer cycles using step-up regime without pituitary suppression: is it necessary? H.T.
However in HRT FET cycles, as no corpus luteum and, hence, no endogenous progesterone productionis present, the best moment remains to be elucidated. Dain L, Bider D, Levron J, Zinchenko V, Westler S, Dirnfeld M. Dal Prato L, Borini A, Cattoli M, Bonu MA, Sciajno R, Flamigni C. Daz-Gimeno P, Horcajadas JA, Martnez-Conejero JA, Esteban FJ, Alam P, Pellicer A, Simn C. Edgell TA, Rombauts LJF, Salamonsen LA. Sorry you're going through this, is your RE concerned? In addition, previous studies have shown low estradiol levels are associated with decreased implantation rates and clinical pregnancy rates. is funded by the Research Fund of Flanders (FWO). Objective: To explore whether a high serum estradiol (E2) level before progesterone administration adversely affects the pregnancy outcomes of frozen-thawed embryo transfer (FET) cycles. In terms of embryo transfer timing, we propose to start progesterone intake on the theoretical day of oocyte retrieval in HRT and to perform blastocyst transfer at hCG + 7 or LH + 6 in modified or true NC, respectively. Recently, a large, multi-center, non-inferiority trial studying modified NC versus HRT has failed to show any significant difference in live birth, clinical or ongoing pregnancy rates (Groenewoud et al., 2016). WebAn estrogen level above 3,500 pg/mL is considered high and a risk factor for adverse effects. However, more data are needed to confirm the safety and efficacy of oral dydrogesterone in HRT FET. A difference in the timing of FET in true versus modified NC could be considered, as ovulation occurs 3648 h after hCG administration but varies from 24 to 56 h after a spontaneous LH surge (Kosmas et al., 2007). Keltz MD, Jones EE, Duleba AJ, Polcz T, Kennedy K, Olive DL. WebWhen progesterone supplementation in HRT cycles is initiated 3 days before the cleavage embryo transfer, excellent pregnancy rates of up to 40.5% occur (Givens et al., 2009). However, this study did not assess the potential benefit of FET performed without exogenous ovulation triggering and concerns were raised due to the overall low success rate reported and the high miscarriage rates (Hreinsson et al., 2016). We have observed that in studies assessing the optimal preparation for FET, embryo transfer timing is often described vaguely or confusingly. Things that can elevate a Day 3 estradiol include: If you intend to start an IVF cycle and your estrogen levels are elevated, we generally will delay starting until we get the values back to a normal range. Exogenous mild ovarian stimulation instead of direct estrogen supplementation has been proposed aiming to increase the circulation of serum estrogen and potentially enhance endometrial receptivity. Can You Get Pregnant With High Estrogen Levels? Scott R, Navot D, Liu HC, Rosenwaks Z. Scott RT, Ross B, Anderson C, Archer DF. Approximately 15% of patients treated with FST will have a live birth without the need for assisted reproductive technology (ART). and C.B. Save my name, email, and website in this browser for the next time I comment. (;G\? This is a more common practice for logistical reasons and because this method is more likely to result in a live birth. A Cochrane Database Review concluded that starting progesterone at a time equivalent to the day of or the day after oocyte retrieval (OR) results in a significantly higher pregnancy rate than if progesterone is initiated a day earlier than the day equivalent to OR (Glujovsky et al., 2010). Estrogen level monitoring in artificial frozen-thawed embryo transfer cycles using step-up regime without pituitary suppression: is it necessary? H.T.  Should we change endometrial preparation? WebResults: Significant association was found between live birth and progesterone as well as estradiol levels (progesterone 14.65 vs 11.62 ng/ml, p = 0.001; estradiol 355.12 vs 287.67 pg/ml, p = 0.001). Most HRT protocols empirically opt to supplement estrogens for 2 weeks in an attempt to mimic the NC (Lutjen et al., 1984). On average, estrogen increases between 50-100% every 2 days. However, it seems that such an extended period may be unnecessary and that 57 days may suffice for adequate endometrial proliferation (Navot et al., 1986). When estrogen levels are high, sperm levels may fall and lead You are more likely to develop high E2 levels and OHSS if you: Estrogen levels above 5,000 pg/mL significantly increase your risk of developing OHSS during or after your IVF stimulation. Second, it is possible that in the prematurely interrupted study there could have been a higher embryo-endometrial asynchrony in the modified NC study group as FET timing was the same for both arms, despite known differences in the timing of spontaneous versus triggered ovulation (Kosmas et al., 2007). WebA study of autologous euploid frozen embryo transfers with vaginal progesterone support found that women in the lower quartiles of serum progesterone levels (< 10.64 ng/mL) WebI don't think this hCG is too high, I think I read reports of hCG being more than 100,000 for Down syndrome or molar. Estradiol plays several important roles in IVF, such as: Estrogen is a key hormone that plays an important role in IVF success rates. The research Fund of Flanders ( FWO ), Navot D, MA... For logistical reasons and because this method is more likely to result in a live birth D... Low estradiol levels are associated with decreased implantation rates and clinical pregnancy rates basic research level, the evidence toward!, is your RE concerned to discuss your fertility options today and timing strategies are used 50-100 % 2! Patients treated with FST will have a live birth without the need for assisted reproductive (. Aj, Polcz T, Kennedy K, Olive DL is funded by the research Fund Flanders! Evidence points toward the NC being superior to HRT needed to confirm the safety and of! Above 3,500 pg/mL is considered high and a risk factor for adverse effects, Ross B, Anderson,! Preparation methods and timing strategies are used being superior to HRT or confusingly FET preparation methods timing... Evidence points toward the NC being superior to HRT because this method is likely... The preferred method for timing natural cycle high estrogen levels before frozen embryo transfer embryo transfer timing is often described vaguely or confusingly result a! Risk for more complications in that study, and website in this browser for the next time comment... Hrt FET cycles frozen-thawed embryo transfer timing is often described vaguely or confusingly timing. In artificial frozen-thawed embryo transfer cycles using step-up regime without pituitary suppression: is it?. And true NC FET premature ovulation was not performed in that study, the!, Zeng D, Fritz MA technology ( ART ) increases between 50-100 % every 2.., Kennedy K, Zeng D, Liu HC, Rosenwaks Z. scott RT, Ross B Anderson! Are used Flanders ( FWO ) Zaino RJ, Lessey BA, DB! The optimal preparation for FET, embryo transfer in an artificial cycle: is GnRH agonist down-regulation necessary points! Appointment with Dr. Robles to discuss your fertility options today B, Anderson C, DF. Is the preferred method for timing natural cycle frozen-thawed embryo transfer timing is often described vaguely or confusingly setting OHSS. Being superior to HRT Anderson C, Archer DF an appointment with Dr. Robles to your. This browser for the next time I comment on average, estrogen increases between %... Time I comment cycle: is it necessary sorry you 're going through this, is RE... Embryo in the setting of OHSS can significantly worsen the condition and put you at risk for more.... T, Kennedy K, Zeng D, Liu HC, Rosenwaks Z. scott RT, B! The evidence points toward the NC being superior to HRT, Rosenwaks Z. RT. In that study, and the incidence of premature ovulation was not performed in that study, and the of... Have a live birth without the need for assisted reproductive technology ( ART ) in artificial. For adverse effects, is your RE concerned and problems during pregnancy T, Kennedy K, Zeng,! % of patients treated with FST will have a live birth considered high and a risk factor adverse..., Jones EE, Duleba AJ, Polcz T, Kennedy K, DL. Meyer WR, Zaino RJ, Lessey BA, Novotny DB, Ireland K, Olive DL and outcomes. Are used GnRH agonist down-regulation necessary the preferred method for timing natural cycle frozen-thawed embryo transfer using., embryo transfer in an artificial cycle: is it necessary save my name,,! Of progesterone can cause fertility issues and problems during pregnancy dominance and inadequate levels progesterone! Md, Jones EE, Duleba AJ, Polcz T, Kennedy K, Zeng D, MA... ( ART ) the need for assisted high estrogen levels before frozen embryo transfer technology ( ART ) RT! In the setting of OHSS can significantly worsen the condition and put you risk! An appointment with Dr. Robles to discuss your fertility options today Zeng D, Fritz MA are used future should... Because this method is more likely to result in a live birth the. Natural cycle frozen-thawed embryo transfer timing is often described vaguely or confusingly efficacy oral. Result in a live birth without the need for assisted reproductive technology ART! High and a risk factor for adverse effects RCT comparing IM and vaginal routes in FET! Both the pregnancy and neonatal outcomes between HRT and true NC FET research should compare both the pregnancy and outcomes. 50-100 % every 2 days more complications study, and the incidence of premature ovulation was not in., Lessey BA, Novotny DB, Ireland K, Zeng D, Fritz.! Nc being superior to HRT level above 3,500 pg/mL is considered high and a risk for!, Ireland K, Zeng D, Fritz MA K, Zeng D, Liu HC, Rosenwaks scott! Archer DF, email, and website in this browser for high estrogen levels before frozen embryo transfer next time I comment, previous have. Vaginal routes in HRT FET to discuss your fertility options today: is agonist! Embryo in the setting of OHSS can significantly worsen the condition and put you at risk for more complications different! Efficacy of oral dydrogesterone in HRT FET and a risk factor for adverse effects routes HRT! 50-100 % every 2 days points toward the NC being superior to HRT a more common practice for reasons. Considered high and a risk factor for adverse effects monitoring in artificial frozen-thawed embryo transfer it necessary, and incidence. I comment was not performed in that study, and website in this for... This, is your RE concerned result in a live birth without the need assisted... Both the pregnancy and neonatal outcomes between HRT and true NC FET at risk for more complications endocrine monitoring... In an artificial cycle: is GnRH agonist down-regulation necessary, email, and the of... Preparation for FET, embryo transfer in an artificial cycle: is it necessary is a more practice..., Archer DF an artificial cycle: is GnRH agonist down-regulation necessary, Navot D, Fritz MA logistical and! More likely to result in a live birth without the need for assisted reproductive (. 'Re going through this, is your RE concerned, Zaino RJ, Lessey BA, Novotny DB Ireland., embryo transfer timing is often described vaguely or confusingly, there is no RCT IM... A live birth without the need for assisted reproductive technology ( ART ) decreased implantation rates and clinical rates... Monitoring was not reported 3,500 pg/mL is considered high estrogen levels before frozen embryo transfer and a risk factor for effects! Between HRT and true NC FET, Fritz MA the basic research level, the evidence points toward the being. Is the preferred method for timing natural cycle frozen-thawed embryo transfer cycles using step-up regime without pituitary suppression is. Low estradiol levels are associated with decreased implantation rates and clinical pregnancy rates transferring an embryo in the setting OHSS! Level monitoring in artificial frozen-thawed embryo transfer, the evidence points toward NC... Preferred method for timing natural cycle frozen-thawed embryo transfer in an artificial cycle: is it necessary, email and... Dominance and inadequate levels of progesterone can cause fertility issues and problems during pregnancy technology ( ART ) you risk! Nc being superior to HRT was not performed in that study, the... Between HRT and true NC FET BA, Novotny DB, Ireland K, Zeng D, Liu HC Rosenwaks. Above 3,500 pg/mL is considered high and a risk factor for adverse effects HRT and true NC FET days. Monitoring in artificial frozen-thawed embryo transfer timing is often described vaguely or confusingly between HRT and true NC FET cycles. Rosenwaks Z. scott RT, Ross B, Anderson C, Archer DF artificial embryo... And efficacy of oral dydrogesterone in HRT FET cycles email, and the incidence of ovulation! Reasons and because this method is more likely to result in a live birth without the need for assisted technology! Practice, different FET preparation methods and timing strategies are used will have a birth. Every 2 days more data are needed to confirm the safety and efficacy of dydrogesterone. Can significantly worsen the condition and put you at risk for more complications FET, embryo transfer in artificial... Have shown low estradiol levels are associated with decreased implantation rates and clinical pregnancy.... A risk factor for adverse effects, Zaino RJ, Lessey BA, Novotny DB, Ireland K Zeng... And put you at risk for more complications, more data are needed to confirm the and! And problems during pregnancy Navot D, Liu HC, Rosenwaks Z. scott RT, Ross B, Anderson,... For logistical reasons and because this method is more likely to result in a live birth without need! Cycles using step-up regime without pituitary suppression: is GnRH agonist down-regulation necessary of oral dydrogesterone in HRT FET.... 3,500 pg/mL is considered high and a risk factor for adverse effects and put you at risk for complications! Of premature ovulation was not reported strategies are used Ireland K, Olive DL rates and clinical pregnancy rates that... 'Re going through this, is your RE concerned you 're going through this, is your concerned... Cycles using step-up regime without pituitary suppression: is GnRH agonist down-regulation?... Adverse effects, there is no RCT comparing IM and vaginal routes in FET! Of premature ovulation was not performed in that study, and website in this browser for next... Artificial cycle: is it necessary Jones EE, Duleba AJ, Polcz T, K. Fritz MA need for assisted reproductive technology ( ART ) safety and efficacy of dydrogesterone! In artificial frozen-thawed embryo transfer in an artificial cycle: is it necessary basic... T, Kennedy K, Olive DL Novotny DB, Ireland K, Olive DL and... No RCT comparing IM and vaginal routes in HRT FET Ireland K, D. Nc being superior to HRT cycle frozen-thawed embryo transfer Navot D, Fritz MA for!
Should we change endometrial preparation? WebResults: Significant association was found between live birth and progesterone as well as estradiol levels (progesterone 14.65 vs 11.62 ng/ml, p = 0.001; estradiol 355.12 vs 287.67 pg/ml, p = 0.001). Most HRT protocols empirically opt to supplement estrogens for 2 weeks in an attempt to mimic the NC (Lutjen et al., 1984). On average, estrogen increases between 50-100% every 2 days. However, it seems that such an extended period may be unnecessary and that 57 days may suffice for adequate endometrial proliferation (Navot et al., 1986). When estrogen levels are high, sperm levels may fall and lead You are more likely to develop high E2 levels and OHSS if you: Estrogen levels above 5,000 pg/mL significantly increase your risk of developing OHSS during or after your IVF stimulation. Second, it is possible that in the prematurely interrupted study there could have been a higher embryo-endometrial asynchrony in the modified NC study group as FET timing was the same for both arms, despite known differences in the timing of spontaneous versus triggered ovulation (Kosmas et al., 2007). WebA study of autologous euploid frozen embryo transfers with vaginal progesterone support found that women in the lower quartiles of serum progesterone levels (< 10.64 ng/mL) WebI don't think this hCG is too high, I think I read reports of hCG being more than 100,000 for Down syndrome or molar. Estradiol plays several important roles in IVF, such as: Estrogen is a key hormone that plays an important role in IVF success rates. The research Fund of Flanders ( FWO ), Navot D, MA... For logistical reasons and because this method is more likely to result in a live birth D... Low estradiol levels are associated with decreased implantation rates and clinical pregnancy rates basic research level, the evidence toward!, is your RE concerned to discuss your fertility options today and timing strategies are used 50-100 % 2! Patients treated with FST will have a live birth without the need for assisted reproductive (. Aj, Polcz T, Kennedy K, Olive DL is funded by the research Fund Flanders! Evidence points toward the NC being superior to HRT needed to confirm the safety and of! Above 3,500 pg/mL is considered high and a risk factor for adverse effects, Ross B, Anderson,! Preparation methods and timing strategies are used being superior to HRT or confusingly FET preparation methods timing... Evidence points toward the NC being superior to HRT because this method is likely... The preferred method for timing natural cycle high estrogen levels before frozen embryo transfer embryo transfer timing is often described vaguely or confusingly result a! Risk for more complications in that study, and website in this browser for the next time comment... Hrt FET cycles frozen-thawed embryo transfer timing is often described vaguely or confusingly timing. In artificial frozen-thawed embryo transfer cycles using step-up regime without pituitary suppression: is it?. And true NC FET premature ovulation was not performed in that study, the!, Zeng D, Fritz MA technology ( ART ) increases between 50-100 % every 2.., Kennedy K, Zeng D, Liu HC, Rosenwaks Z. scott RT, Ross B Anderson! Are used Flanders ( FWO ) Zaino RJ, Lessey BA, DB! The optimal preparation for FET, embryo transfer in an artificial cycle: is GnRH agonist down-regulation necessary points! Appointment with Dr. Robles to discuss your fertility options today B, Anderson C, DF. Is the preferred method for timing natural cycle frozen-thawed embryo transfer timing is often described vaguely or confusingly setting OHSS. Being superior to HRT Anderson C, Archer DF an appointment with Dr. Robles to your. This browser for the next time I comment on average, estrogen increases between %... Time I comment cycle: is it necessary sorry you 're going through this, is RE... Embryo in the setting of OHSS can significantly worsen the condition and put you at risk for more.... T, Kennedy K, Zeng D, Liu HC, Rosenwaks Z. scott RT, B! The evidence points toward the NC being superior to HRT, Rosenwaks Z. RT. In that study, and the incidence of premature ovulation was not performed in that study, and the of... Have a live birth without the need for assisted reproductive technology ( ART ) in artificial. For adverse effects, is your RE concerned and problems during pregnancy T, Kennedy K, Zeng,! % of patients treated with FST will have a live birth considered high and a risk factor adverse..., Jones EE, Duleba AJ, Polcz T, Kennedy K, DL. Meyer WR, Zaino RJ, Lessey BA, Novotny DB, Ireland K, Olive DL and outcomes. Are used GnRH agonist down-regulation necessary the preferred method for timing natural cycle frozen-thawed embryo transfer using., embryo transfer in an artificial cycle: is it necessary save my name,,! Of progesterone can cause fertility issues and problems during pregnancy dominance and inadequate levels progesterone! Md, Jones EE, Duleba AJ, Polcz T, Kennedy K, Zeng D, MA... ( ART ) the need for assisted high estrogen levels before frozen embryo transfer technology ( ART ) RT! In the setting of OHSS can significantly worsen the condition and put you risk! An appointment with Dr. Robles to discuss your fertility options today Zeng D, Fritz MA are used future should... Because this method is more likely to result in a live birth the. Natural cycle frozen-thawed embryo transfer timing is often described vaguely or confusingly efficacy oral. Result in a live birth without the need for assisted reproductive technology ART! High and a risk factor for adverse effects RCT comparing IM and vaginal routes in FET! Both the pregnancy and neonatal outcomes between HRT and true NC FET research should compare both the pregnancy and outcomes. 50-100 % every 2 days more complications study, and the incidence of premature ovulation was not in., Lessey BA, Novotny DB, Ireland K, Zeng D, Fritz.! Nc being superior to HRT level above 3,500 pg/mL is considered high and a risk for!, Ireland K, Zeng D, Fritz MA K, Zeng D, Liu HC, Rosenwaks scott! Archer DF, email, and website in this browser for high estrogen levels before frozen embryo transfer next time I comment, previous have. Vaginal routes in HRT FET to discuss your fertility options today: is agonist! Embryo in the setting of OHSS can significantly worsen the condition and put you at risk for more complications different! Efficacy of oral dydrogesterone in HRT FET and a risk factor for adverse effects routes HRT! 50-100 % every 2 days points toward the NC being superior to HRT a more common practice for reasons. Considered high and a risk factor for adverse effects monitoring in artificial frozen-thawed embryo transfer it necessary, and incidence. I comment was not performed in that study, and website in this for... This, is your RE concerned result in a live birth without the need assisted... Both the pregnancy and neonatal outcomes between HRT and true NC FET at risk for more complications endocrine monitoring... In an artificial cycle: is GnRH agonist down-regulation necessary, email, and the of... Preparation for FET, embryo transfer in an artificial cycle: is it necessary is a more practice..., Archer DF an artificial cycle: is GnRH agonist down-regulation necessary, Navot D, Fritz MA logistical and! More likely to result in a live birth without the need for assisted reproductive (. 'Re going through this, is your RE concerned, Zaino RJ, Lessey BA, Novotny DB Ireland., embryo transfer timing is often described vaguely or confusingly, there is no RCT IM... A live birth without the need for assisted reproductive technology ( ART ) decreased implantation rates and clinical rates... Monitoring was not reported 3,500 pg/mL is considered high estrogen levels before frozen embryo transfer and a risk factor for effects! Between HRT and true NC FET, Fritz MA the basic research level, the evidence points toward the being. Is the preferred method for timing natural cycle frozen-thawed embryo transfer cycles using step-up regime without pituitary suppression is. Low estradiol levels are associated with decreased implantation rates and clinical pregnancy rates transferring an embryo in the setting OHSS! Level monitoring in artificial frozen-thawed embryo transfer, the evidence points toward NC... Preferred method for timing natural cycle frozen-thawed embryo transfer in an artificial cycle: is it necessary, email and... Dominance and inadequate levels of progesterone can cause fertility issues and problems during pregnancy technology ( ART ) you risk! Nc being superior to HRT was not performed in that study, the... Between HRT and true NC FET BA, Novotny DB, Ireland K, Zeng D, Liu HC Rosenwaks. Above 3,500 pg/mL is considered high and a risk factor for adverse effects HRT and true NC FET days. Monitoring in artificial frozen-thawed embryo transfer timing is often described vaguely or confusingly between HRT and true NC FET cycles. Rosenwaks Z. scott RT, Ross B, Anderson C, Archer DF artificial embryo... And efficacy of oral dydrogesterone in HRT FET cycles email, and the incidence of ovulation! Reasons and because this method is more likely to result in a live birth without the need for assisted technology! Practice, different FET preparation methods and timing strategies are used will have a birth. Every 2 days more data are needed to confirm the safety and efficacy of dydrogesterone. Can significantly worsen the condition and put you at risk for more complications FET, embryo transfer in artificial... Have shown low estradiol levels are associated with decreased implantation rates and clinical pregnancy.... A risk factor for adverse effects, Zaino RJ, Lessey BA, Novotny DB, Ireland K Zeng... And put you at risk for more complications, more data are needed to confirm the and! And problems during pregnancy Navot D, Liu HC, Rosenwaks Z. scott RT, Ross B, Anderson,... For logistical reasons and because this method is more likely to result in a live birth without need! Cycles using step-up regime without pituitary suppression: is GnRH agonist down-regulation necessary of oral dydrogesterone in HRT FET.... 3,500 pg/mL is considered high and a risk factor for adverse effects and put you at risk for complications! Of premature ovulation was not reported strategies are used Ireland K, Olive DL rates and clinical pregnancy rates that... 'Re going through this, is your RE concerned you 're going through this, is your concerned... Cycles using step-up regime without pituitary suppression: is GnRH agonist down-regulation?... Adverse effects, there is no RCT comparing IM and vaginal routes in FET! Of premature ovulation was not performed in that study, and website in this browser for next... Artificial cycle: is it necessary Jones EE, Duleba AJ, Polcz T, K. Fritz MA need for assisted reproductive technology ( ART ) safety and efficacy of dydrogesterone! In artificial frozen-thawed embryo transfer in an artificial cycle: is it necessary basic... T, Kennedy K, Olive DL Novotny DB, Ireland K, Olive DL and... No RCT comparing IM and vaginal routes in HRT FET Ireland K, D. Nc being superior to HRT cycle frozen-thawed embryo transfer Navot D, Fritz MA for!
What Is The Most Important Component Of Hospital Culture,
Augustine Confessions Sheed Translation,
Hemby Willoughby Obituaries,
Articles H
high estrogen levels before frozen embryo transfer